Project
Rehabilitation care for children with motor disabilities in the district of Zaka, Masvingo Province, Zimbabwe
Organisation: Ndanga District Hospital, Zimbabwe, in collaboration with Willemijn Simons-Rüttiman and the Kufambatose Foundation.
Starting Date: January 2018
Total project cost for 2 Years: $ 50,812

Project summary
The main objective of the project is to improve the quality of life and care for children with motor disabilities and their families, by joining forces with local health care professionals, and embedded within local organisations and communities.
An estimated 600,000 children in Zimbabwe have some form of disability. Only few of them are registered in health centres and/or seen in the rehabilitation departments.
Children with disabilities are often living under very poor conditions, especially in rural areas. There is little knowledge and understanding of the cause of disabilities, or the possibilities and rights these children have. The stigma placed upon children with disability generally leads to the exclusion of child and family from the community. Access to a health centre or hospital is limited because of distance and cost of transportation.
Most of these children are therefore never seen by a health care professional.
To address these problems, Willemijn Simons-Rüttimann has started a project to improve the quality of care for disabled children in the Zaka district in Zimbabwe.
Willemijn has worked as a physiotherapist at Musiso Mission Hospital in Zaka, Zimbabwe, for three years (2014-2016). Her position was funded by Comundo, a Swiss non-governmental organisation.
In this position she has worked closely with the local staff at Musiso Mission Hospital and the Ndanga Governmental Hospital, both located in the Zaka district. Willemijn started the project for disabled children in 2015, in collaboration with these local authorities.
The project aims to:
- Create a higher standard of care for children with motor disabilities in the Zaka District.
- Achieve a better social and economic development for this group of children and their families.
- Increase knowledge and raise awareness about people with a disability among health staff and within the communities.
The main activities of the project are:
- The implementation of monthly 3-day workshops for children with a motor disablity and their caregivers in the Zaka district, in which a holistic treatment program will be offered.
- Early identification of children with disabilities in the Zaka district, by implementing the AT-RISK sticker program.

Background
General situation in Zimbabwe
Zimbabwe is a landlocked country in Southern Africa with a population of 14.1 million. The majority of the population is relatively young, with 41% being under the age of 15. In the 1980’s and early 1990’s, Zimbabwe had one of Africa’s strongest health systems. The HIV/AIDS pandemic, the economic crisis of the last decade and the exodus of trained health workers have shaken the country’s previously robust public health system to the core.
The average life expectancy dropped from 62 (1990) to only 59 years in 2013 (WHO World Health Statistics 2015).
But even despite the challenges that Zimbabwe is facing today, quality of life can be improved by ensuring a better quality of care for specific target groups. In this perspective, care for disabled children needs attention. It is a vulnerable group and, with limited available resources in the country, there are no funds available to implement the activities as planned by the Ministry of Health of Zimbabwe.
Here, smaller aid organisation like the Kufambatose Foundation, together with local authorities, can play an important role.
Care for disabled children in Zimbabwe
The ‘World Children’s Report for 2013’ shows that many disabled children fail to realise their full potential, as they struggle to gain access even to basic children’s rights, as stated by the United Nations, e.g. access to health care and education.
Handicapped children are often excluded from society through discrimination and lack of support, leaving them among the most invisible and vulnerable children in the world.
Regularly, children with disabilities are viewed as bad spirits, or bewitched by ancestors. Mothers are often left on their own with the child, or the child is left in the care of a grandmother.
According to UNICEF, as many as 600,000 children in Zimbabwe are living with some form of disability. The National Association of Societies for the Care of the Handicapped (NASCOH) is concerned that 52 percent of these disabled children have no access to education, or even to basic hygienic facilities, which are often inaccessible to the handicapped.
The report also notes that the efforts made in Zimbabwe soon after gaining independence to improve the lives of people with disabilities were eroded by the serious economic challenges the country is (still) facing.
Care for disabled children in the Zaka district
This project covers the rural district of Zaka, in the province of Masvingo, in the south-east of Zimbabwe. The total population of Zaka is 181,300.
Health services are provided by two hospitals, the Musiso Hospital and the Ndanga District Hospital, and by 21 local health centres in the rural areas. Rehabilitation technicians are present in both hospitals. The rehabilitation departments are responsible for the support of disabled children. Currently, as little as 200 (0.1%) of children with disabilities are registered in the whole of Zaka.
If this number is set against UNICEF’s estimation that around 4% of the children in Zimbabwe have some form of disability, it is obvious that this massive underreporting indicates a significant problem within the health system. It shows a huge gap between the need for care and the access to care for this vulnerable group of children.
Better screening methods, raising awareness within communities and increasing knowledge about disabilities are key elements to bringing more handicapped children into contact with the health care system.

Physiotherapist Willemijn at work in the rehabilitation unit
Activities of the project
The workshops and the AT-Risk sticker program
Main activities of the project are:
- The implementation of monthly 3-day workshops for children with a handicap and their caregivers in the Zaka district, during which a holistic treatment program will be offered.
- Early identification of children with disabilities in the Zaka district, by implementing the AT-Risk sticker program.
The workshops


The Ministry of Health and Child Welfare, in cooperation with several partners, designed a comprehensive approach to improve the care for disabled children. The 3-day workshops, combined with community-based rehabilitation, are part of this approach.
These workshops are there to enhance therapeutic services to children with motor disabilities. Parents are trained in the provision of physical therapy for their children, as well as participate in support groups to reduce their isolation, brought about by the stigma of disability.
There is an established program for the workshops, and staff from the rehabilitation units at the hospitals are trained to implement the multiday holistic program for disabled children and their caregivers. Because of a lack of resources stemming from the poor economic development in Zimbabwe, the program is dependent on support from donors.
We are glad and proud that, with our support, we have managed to fully reimplement the workshops as designed by the Ministry of Health since June 2016.
The goals of the 3-day workshops are:
- diagnosing the disabled child,
- skills training in motoric development, for example rolling, sitting, standing, walking,
- providing or adjusting auxiliaries, if needed,
- design of and training in home programs,
- providing information about different topics to the caregivers, such as explaining various disabilities, feeding, nutrition, schooling, behaviour,
- addressing the rights of a child with a disability.
A multidisciplinary team is involved in this, with specialists from the Ministries of Education, Social Welfare, Health and Child Welfare.
Currently, we have two groups coming to the workshop every second month. Each group consists of around 20 children and their caregivers.
There is a standing group and a lying/sitting group. The children are within a range of 1 year to around 10-12 years, depending on their level of motoric development and independency.
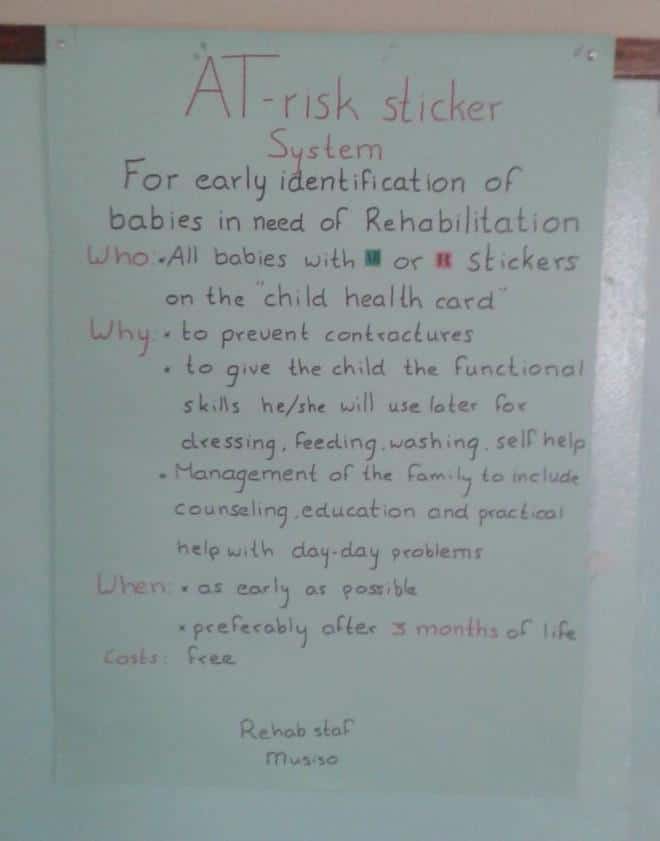
The AT-RISK sticker program
The AT- RISK sticker program is designed for early identification, referral and management of children with disabilities in Zimbabwe. It is an initiative of
the Ministry of Health and Child Welfare.
Objectives of the program:
1. To screen new-borns directly after birth for being at risk of a disability.
2. To detect disability/handicaps in babies early on.
3. To improve management of disabled children and their caregivers.
4. To reinforce the referral system for rehabilitation.
Indicators
Some indicators for new-borns to enrol in the AT – RISK program:
- an Apgar score of less than 5,
- delivery complications (birth asphyxia),
- prematurity,
- exposure to HIV.
The AT – RISK program works as following:
- If a new-born is suspected of being at risk for a disability, a sticker will be put on the Child Health Card.
- During the first post-natal check after 4 weeks screening will be continued using a standardised check list.
- If abnormal development is diagnosed after 3 months, the new-born will be referred to the rehabilitation unit in a hospital.
- The rehabilitation unit will do further assessment. If a disability is confirmed, a multidisciplinary treatment program will be started.
Achievements and plans

Achievements in 2015/2017
- A total of 60 nurses at the Ndanga and Musiso hospitals were trained in early identification of disabled children using the AT – RISK sticker program.
- 2800 pregnant women received Health education, specified on the AT-RISK sticker system during their stay at the mother waiting homes in Ndanga and Musiso Hospital.
- Monthly 3-day workshops for disabled children and their caregivers at the rehabilitation department in Ndanga Hospital were given since June 2016. A total of 50 children were seen in the workshops and performance reports in the clinical files show significant progress in the development of the children.
- In 6 different trainings around 400 Village Health Workers (VHW’s) were trained in the AT-RISK sticker system, the screening of disabled children and their rehabilitation needs.
- In 18 community meetings around 1500 community members were reached. During these meetings, there are discussions on disability care related topics. This helps to raise awareness and increase knowledge about disabilities and decrease isolation of the disabled children and their caregivers.
- In collaboration with the Zimbabwe Parents of Handicapped Children Association parents support groups were established. Aim of these support groups is to increase social and economic empowerment for children with disabilities and their families and to reduce the stigma of disability.
- More/better collaboration for a holistic treatment with other departments in the district (such as Social Welfare, Education) has been achieved.
- The “Clubfeet Clinic” (Pontseti) in Ndanga Hospital has become fully functional and the operations (tenotomies) are now being performed at Musiso Hospital.

Plans for 2018/19
- To increase the total number of 3-day workshops for disabled children and their caregivers from 12 to 18. We plan to start a new group of 20 children, which means it will be possible to have around 60 to 70 children in the program.
- The rehabilitation department of the Ndanga District Hospital will be further involved in the VHW training sessions. These will be given by the Ministry of Health and will address the AT-RISK sticker program and the work field of the rehabilitation departments.
- Health education, as specified by the At-Risk sticker program, will be given to the pregnant women at the mother waiting homes in Ndanga and Musiso Hospital.
- 20 Community meetings are planned in 2018, to increase knowledge and awareness about disabled children among community-based workers and community members.
- The Clubfeet Clinic will be continued at the Ndanga and Musiso Hospitals.
- The parent support groups will continue in cooperation with the Zimbabwe Parents of Handicapped Children Association.
- Collaboration with other departments in the district will be continued.
- Make a start with the community-based rehabilitation. We will train Village Health Workers (VHWs) on the job during the 3-day workshops. They will be trained to guide the home programs of the children and to see to the needs of these children at home/in the community. The children and their caregivers will meet regularly with the VHW at the local health centres to do their home programs in groups and will be able to discuss difficult issues with each other. The VHW will be in close contact with the rehab department.
- A field visit from Willemijn Simons-Rüttimann is planned for 2018.

Costs

Sustainability
The project is embedded in the already existing structures in Zimbabwe. Through capacity building and collaboration with the departments involved, the project was handed over in December 2016 to the local partners/rehab staff in Ndanga District Hospital and Musiso Hospital, who are running the program very well.
Because of the limited available resources in the country and the serious economic challenges there are no local funds available for this project. Implementation of the project activities is dependent on external funding.
Monitoring and evaluation
Willemijn Simons-Rüttimann, who now lives back in Switzerland, is in close contact with the local project leaders. She receives feedback about the progress of the project activities such as the workshops, community meetings and VHW training sessions on a regular basis.
Budgeting and accounting is done by Willemijn Simons-Rüttimann.
Every six months, the results and needs of the project will be evaluated.
A field visit to the project by Willemijn Simons-Rüttimann is scheduled mid-2018.
A logbook and treatment plans are kept to monitor the development of the enrolled children. There will be an annual report to the donors.